KSL Investigates: How COVID-19 Treatments Have Changed In Nine Months
Dec 10, 2020, 10:41 PM | Updated: Jun 19, 2022, 9:57 pm

SALT LAKE CITY, Utah — March 6, 2020, saw the first confirmed case of COVID-19 in Utah.
In the nine months since, we are still learning how COVID-19 affects people and how best to treat the disease. No one more than the frontline doctors and nurses treating patients in crowded ICUs.
“We are very, very stretched,” said Dr. Sean Callahan, assistant professor of internal medicine at the University of Utah School of Medicine’s Division of Pulmonary and Critical Care. He has been treating COVID-19 patients since March.
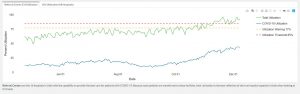
ICU utilization at Utah’s 16 referral hospitals, which are better equipped to treat COVID-19 patients. (Utah Dept. of Health)
“It was quite scary, to be honest,” he recalled. “We had this emerging virus that we didn’t know how to take care of. The novelty of it made it very difficult for us to know how to treat patients.”
Learning What Treatments Work & Which Do Not
Since then, he said many of the treatments for COVID have changed. “A lot of the things that we were doing back in March, springtime, we don’t do anymore,” Callahan said.
Things like giving hydroxychloroquine — once thought to help but has been deemed unhelpful nearly universally.



Doctors are also being more judicious with when to intubate a patient. “There was a push toward earlier intubation, so putting people on ventilators earlier on, which we have abandoned that strategy,” said Callahan.
“Back in the day, there was a lot of concern that people were hurting themselves having to breathe so hard, or it was inevitable they would end up on the ventilator so why not just do it earlier on?” he said. “We found that is not the case at all so early intubation is not necessary. We’ll usually intubate patients when it’s the clinical right thing to do.”
Current & Future COVID Treatments
Now, doctors have been more widely using steroids to help ease symptoms, along with antiviral drug Remdesivir. It’s a drug President Donald Trump received as part of his treatment for COVID-19 earlier this year.
Additional treatments are still being fine-tuned, including the use of blood-thinning agents and therapies similar to steroids that calm aggravated immune systems.
“We know that some patients get really sick as a result of the immune system kind of going haywire, going berserk,” said Callahan. “That’s part of the reason for steroids is thinking they’re helpful for those patients. There are therapies that are like steroids that we think may be beneficial, but we need to investigate further.”
One treatment getting a lot of attention is the use of antibodies, whether manufactured or donated through convalescent plasma.
“There’s a lot of interest in that, and we’re finding there’s probably benefit, but trying to figure out who the right person is at the right time and what severity of disease is something that is rapidly evolving,” he explained. “We’ll probably see more use of that, but we need to figure out when to give those.”
Utahns Surviving COVID-19, But ‘Maimed’
While Utah’s death rate from COVID has been lower than other states’ rates, Callahan says there is great concern about those surviving the disease but with serious health complications.
“A really big concern we have going forward is the amount of weakness and delirium, confusion that patients have after being in the ICU very sick for a long time,” said Callahan. “It’s one of the reasons why you’ll hear us doctors say, ‘mortality rate isn’t everything.’”
Callahan said while most Utahns will survive COVID-19, many leave the ICU not 100% better. The most common symptom is persistent respiratory failure.
“It’s not uncommon that we’ll have people still on a breathing machine for weeks or even months after illness,” he explained. “Even after they leave the hospital, they’ll still need oxygen because their lungs are scarred or damaged.”
Fatigued Staff Means Drop In Care Quality
With a recommendation to the FDA that the Pfizer COVID-19 vaccine be approved for emergency-use authorization Thursday, Callahan said it should be easier now to maintain public health guidelines with an endpoint in sight.
“There is a light at the end of the tunnel. We need people to help us in terms of limiting social interactions through the holidays and to help bridge us to the vaccine,” he said.
Callahan said he averages 80-hour workweeks in the ICU, in addition to many more hours on other rounds. He exclaimed that health care providers are exhausted, which can have negative consequences on care.
“Stretched hospital systems provide worse care,” he said. “I think we are providing great, excellent care at the University of Utah, Intermountain, the VA, everywhere. But mistakes will be made when we are stretched like this.”
Since Nov. 10, referral ICUs, which are the main hospitals best equipped to treat COVID-19 patients, have operated above the 85% capacity threshold for all but two days.
Have you experienced something you think just isn’t right? The KSL Investigators want to help. Submit your tip at investigates@ksl.com or 385-707-6153 so we can get working for you.